
Adaptive yoga for psychological health of children having autism spectrum disorder and with intellectual disability: single case experimental design

Participants
Six children participated along with their caregivers (mothers), recruited from NIEPMD—National Institute for Empowerment of Persons with Multiple Disabilities (Divyangjan), Chennai, Tamil Nadu, India, Under Department of Empowerment of Persons with Disabilities (Divyangjan), Ministry of Social Justice & Empowerment, Govt. of India. The participants are residents and day boarders availing therapeutic services from the institute. Two of the participants attend special model school run by the institute and four attend other schools outside the institute admitted based on special status. The mothers with limited educational background could communicate only in vernacular (Tamil) language and children could follow their mothers. For children, two were non-verbal and other four however verbal, had minimal communication. Mostly caregivers understood them better and helped bridging the communication gaps during the intervention.
The two participants from the institute were introduced to basic yoga postures as part of school curricula in form of a group practice and not formally as a regular therapeutic one-to-one intervention. Other four participants had no prior exposure to yoga. The common therapeutic services like occupational therapy, speech therapy, behavioural therapy and special education were attended time to time by all the participants in the institute.
All the participants are certified by the institute under Department of Empowerment of Persons with Disability (DEPD) gazette guidelines for multiple disability certification on ASD and with ID. As per the guidelines, INCLEN Diagnostic tool for Autism Spectrum Disorder (INDT-ASD) is used by the institute for ASD diagnosis followed by Indian Scale for Assessment of Autism (ISAA) to assess the severity of the condition. The Binet-Kamat Test of Intelligence (BKT) and Malins Intelligence Scale for Indian Children (MISIC) are used to confirm the ID diagnosis and Vineland Social Maturity Scale (VSMS) tool is used assess the severity of the diagnosis.
The inclusion criteria for the study included children those were certified by the institution as multiple disabled having ASD and with ID, chronological age between 7 and 12 years having mild severity level and the caregiver agreed to participate throughout the study. Children having other disabilities, beyond the age criteria, having moderate, severe to profound conditions in ASD and ID were excluded. Demographic details are represented in Table 1. Prior to the participation the informed consent was obtained from parents and/or legal guardians.
The six assessors recruited were practicing clinical psychologists facilitated by the institute. One assessor was mapped to one participant. The trained yoga teacher was the researcher of this study to execute the intervention.
Design
A multiple baseline single case experimental design (AB1B2) was implemented for this study. Each participant went through three phases: (A) baseline phase without intervention, (B1) intervention phase in institute setting with yoga teacher and caregiver, and (B2) intervention phase in home setting with only caregiver. Continuous assessments were planned and administered for each participant at a frequency of every two weeks. The start of the intervention was stratified based on completion of four months of without any yoga practice and completion of associated baseline assessments for respective participants from the time of recruitment. This was planned to establish the existence of the problem related to the variables of interest before start of the intervention. Six months of intervention along with yoga interventionist and caregiver in institute setting followed by three months of yoga along with caregiver alone in home setting was planned. The duration of each intervention phase was decided based on number of intervention sessions as per the plan and that covers at least five counts of assessments for observable data representation for a phase analysis15. The multiple baselines were compared for each replication across six participants, twelve parameters distributed under three psychological domains and two settings. Replication added strength for external validity17. There was limited scope of randomization in this study. The continuous assessment outcomes were blinded for the interventionist and parents, also the assessors were blinded to the intervention procedure throughout the study. The study was conducted and reported as per the Single-Case Reporting Guidelines In Behavioural Interventions (SCRIBE) 2016 Statement18.
The study was approved by Research Committee (RC) of the institution where the study was executed, Doctoral Committee (DC) and Institutional Ethics Committee (IEC) of affiliated University. This is to confirm that all the methods were performed in accordance with the relevant guidelines and regulations as per the Declaration of Helsinki. The study adhered to the approved protocol and consent process.
Intervention procedure
A caregiver orientation workshop was conducted before commencing the intervention to explain the purpose of study and the importance of their role during the intervention. The participants continued their respective regular therapies throughout the study. There were no conditional restrictions on other therapies along with yoga intervention. This also met the purpose of SCED where respective participants served as their own control and only change was additional yoga intervention to assess the impact.
The yoga sessions were administered for the participants as one-to-one intervention along with yoga teacher and caregiver. The intervention sessions started in institute setting along with yoga teacher and caregiver for 120 days, followed by 60 days in home setting along with only caregiver. Each intervention session duration was between 45 to 60 minutes administered every working day of the week excluding weekends and holidays. Before moving from institute setting to home setting, the ownership of intervention was handed over to the caregiver with documented course plan for continuity and smooth execution. A sample documented plan can be referenced in Appendix B.
During home setting phase, six sessions (once in a fortnight) over this period were conducted by the yoga teacher to re-establish the continuity and correct the course plan as applicable. The total days of intervention were adjusted to the planned number of days to compensate any longer absences (more than a week) against medical emergencies. Figure 1 represents the flow.

Course plan
A well-crafted course plan designed that was personalized, prioritized function over form, and was safe based on the fundamental principles of yoga as rooted in the scripture of Patanjali Yogasutra13. (1) Personalized – The practice was designed specific to the individual’s capacity and comfort. The course plan was further modified to suite the physical and mental condition of the participant on a particular day. (2) Function over form – A well-structured yet flexible course plan was designed with appropriate sequences towards fulfilling the function rather than emphasis to achieve the form. (3) Transition of planes were carefully crafted keeping it smooth and in sequence for example from seated to standing to supine to prone to kneeling to seated. (4) For all asanas (physical postures) adequate counter postures were given. (5) Adequate rests were incorporated between asanas integrated with counting or chanting to sustain the participant’s attention. Refer to a sample course plan in Appendix A.
In the initial phase, the sessions were simplified, preparatory, and executed depending on the interest and comfort of the participant on that day. Once the relationship was established (between the yoga teacher and the participant), the nuances were understood by the yoga teacher, the sessions were modified incrementally as per the course plan.
Teaching methodology
The fundamentals of yoga—movement, breath and awareness were achieved by incorporating following adaptation techniques in teaching.
Movement (1) The objective is to get into and come out of the posture with comfort. This sequence was simplified and broken into smaller steps. (2) Adaptations were seasoned by repetition. The approach was iterative and incremental, subject to the readiness of participant for next stage. (3) asana forms were established using patterning wherever applicable with support of caregiver. For example, in dvipada pitham (bridge pose), the hip movements were patterned by support of caregiver lifting the back of the participant.
Breath The breath was influenced in two ways. (1) Our body naturally inhales on expansion and exhales on contraction. Appropriate sequencing by alternating movements helped to achieve the right breathing. (2) Chanting happens on exhalation. Thus, chanting of any syllable of participants’ choice was used in exhalation leading to an implicit inhalation. Length of the chant was moderated as per the participant’s capacity.
Awareness Awareness was brought by maintaining the attention of the participants throughout the session. (1) Every session started by re-establishing a positive connect between yoga teacher, the participant, and the caregiver. (2) The sessions were then executed with continuous engagement in form of movements integrated with limited voice modulated short instructions, counting, chanting, demonstration, and patterning that was suitable for the participant for that session. (3) Every day the teacher assessed the readiness and responsiveness of the participants and accordingly customised the session to bring the best to meet the session objective. (4) The yoga teacher demonstrated and practiced along with the participants throughout the session for ease of imitation.
The visual cues (parallel demonstration), auditory cues (limited voice modulated short instructions), support (caregiver patterning), simple plan integrating movements with chanting or counting; all combined throughout the session helped in making the session mindful and accessible.
Assessments
Indian Scale for Assessment of Autism (ISAA) and Behavioural Assessment Scales for Indian Children with Mental Retardation (BASIC-MR) instruments were used to assess the desired cognitive, behavioural, and emotional parameters objectively.
ISAA is an objective assessment tool for persons with autism which uses observation, clinical evaluation of behaviour, testing by interaction with the subject and information supplemented by parents or caretakers. The ISAA questionnaire is divided under six domains: social relationship and reciprocity, emotional responsiveness, language and communication, behaviour pattern, sensory aspects, and cognitive component. These are further quantified by providing percentages to indicate the frequency, degree and intensity of behavioural characteristics that are observed. Lower the percentage indicates lesser problem and higher the score indicates severity. ISAA is a standardized, reliable, and valid tool for diagnosis and assessment of severity in autism among children19.
BASIC-MR is designed to elicit systematic information on the current level of behaviour in school going children with development disorders. It is developed in two parts. Part-A helps to assess the current level of skills behaviours in the child. Part-B helps to assess the current level of problem behaviours in the child. Part-A consists of seven domains: motor, activity of daily living (ADL), language, reading-writing, number-time, domestic-social, and prevocational-money. Part-B consists of ten domains: violent and destructive behaviour, temper tantrums, misbehaviour with others, self-injurious behaviours, repetitive behaviours, odd behaviours, hyperactive behaviours, rebellious behaviours, antisocial behaviours, and fears. For both Part-A and Part-B each of the respective domains of interest can be consumed independently. The scores for each domain are calculated and converted into a percentage. For Part-A a higher score indicates better skill behaviours, while for Part-B a lower score indicates fewer behaviour problems20.
Twelve domains as variables of interest were picked from ISAA and BASIC-MR (A&B) that was administered to generate percentage scores. The aggregate score of the child on each domain expressed as the raw score. This was converted into percentage for each domain by dividing the obtained raw score by maximum score for that domain and multiplied by 100. The percentage scores across phases were compared against the expected outcome of increasing or decreasing measure as prescribed in the tool. Table 2 describes the assessment parameters of interest, description of problems assessed in each domain, and expected outcome.
The study was conducted over three phases. The assessments were administered by assessors to collect cognitive, behavioural, and emotional data desired for the study every two weeks as per the plan. Total twenty-six (26) assessments were administered throughout the study with first eight during baseline phase (without intervention), followed by twelve during intervention phase in institute setting followed by six during intervention phase in home settings. The assessors were blinded to the intervention modifications. The yoga interventionist and caregivers were blinded to the assessment scores during the intervention phases. After all the assessments were completed and completion of intervention phases, the scores were revealed and consolidated for analysis.
Data analysis–collection, visual and empirical analysis
Overall, 1836 data points generated out of 153 assessments for six participants. The data points were aggregated and analysed for each participant, for each parameter within and across phases. A visual analysis tool was developed using MS Excel to consume the data collected and generate respective participant-parameter wise time sequence line graphs for visualization. Figure 2 represents the sample distribution of 26 data points representing the percentage score on ‘Odd Behaviour’ across three phases for Participant#1. Percentage scores of observable parameters are depicted along the ordinate axis, and the abscissa represents the baseline (B1-B8), intervention institute setting (II1-II12), and intervention home setting (IH1-IH6) assessments.
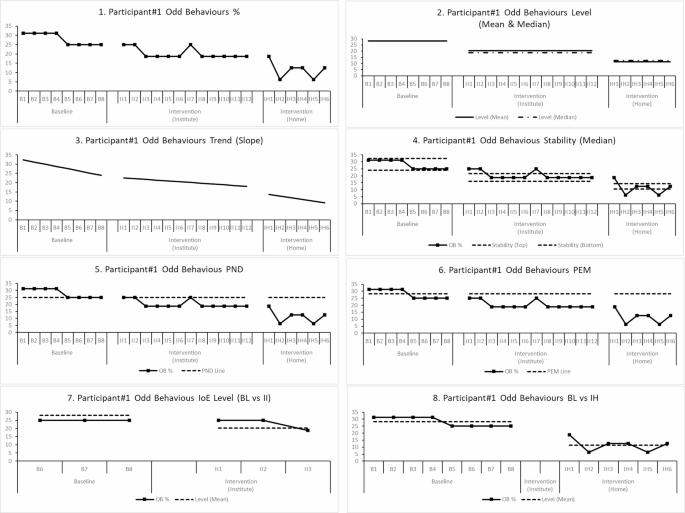
Sample graphs generated for visual analysis for Participant#1 for “odd behaviours” parameter. Description of graphs in order (1) Overall 26 data points across baseline, intervention(institute), intervention(home). (2) Levels represented by Mean and Median Lines. (3) Phase wise trend line. (4) Stability of data between Median range of (+/-) 15%. (5) The Percentage of Non-overlapping data (PND) using min (or max) baseline data point. (6) Percentage of data exceeding median line (PEM). (7) Immediacy of effect comparing last three data points of baseline against first three data points of intervention phase. (8) The level mean comparison between baseline phase and intervention in home setting.
Visual analysis was used to determine the functional relationship between the intervention and observable parameters. A change in percentage score indicates the change in functional behaviour as observed during assessment. If the change is visible to be significant, consistent during visual analysis and aligned to the desired direction, was a clear indication of functional improvement. The visual analysis was further supplemented with quantitative analysis for evaluating the magnitude of impact using multiple non-overlapping indices for effect size and the statistical effect size was calculated using Cohen’s d between baseline to intervention (institute settings) and baseline to intervention (home settings) respectively.
The visual analysis involved evaluating level, trend, and stability of data for within phase analysis. Further the immediacy-of-effect, consistency of data patterns, and non-overlap of data was compared between baseline and respective intervention phases. When the changes (and/or variability) in level, are in the desired direction, are immediate, perceptible, and maintained over time, it is concluded that the changes in behaviour across phases is a result of the intervention and are indicative of functional improvement. This analysis was repeated for all 12 parameters for each participant and across all participants. At least three such demonstration of an intervention effect during visual analysis was necessary for establishing a functional relationship14.
Level, trend, and stability of the data within each phase was evaluated. Mean and median of percentage scores was used to report the level. An increasing or decreasing trend was observed. Within phase stability was evaluated.
by calculating the percentage of data points within 15% of the phase median. The stability criteria are satisfied if about 85% (80-90%) of the data in a phase fall within a 15% range of the median of all data points for that phase.
Between the phase analysis included observing shift in level, change in stability of data distribution, immediacy of effect, and non-overlap of data between phase. The immediacy of effect is observed by change in level, trend or variability comparing the last three data points of baseline compared with first three data points of intervention phase. Immediacy of effect is not considered between baseline and second intervention phase in home settings.
Non overlapping indices were used to calculate the magnitude of effect and quantify the proportion of measurements in the intervention phase not overlapping with the baseline measurements. Non-overlapping of All Pairs (NAP), Percentage of Non-overlapping Data (PND), Percentage of Data Exceeding the Median (PEM) were used to quantify the magnitude of effect to supplement the visual analysis21. This paper depicts the NAP as a parameter to show the magnitude effect. The significance associated with the magnitude of effect was classified as greater than 0.90 are indicative of significant impact, 0.89 to 0.70 represent moderately significant and 0.69 to 0.50 are less significant and score less than 0.50 are considered insignificant21.
The Cohen’s d was used to generate the effect size between baseline and intervention phases (first and second) respectively15. A score greater than 0.80 was considered significant, 0.79 to 0.50 represents moderately significant, 0.49 to 0.20 represent less significant and less than 0.2 is considered insignificant. The polarity of the Cohen’s d represented the alignment to the expected result, negative for decreased effect and positive for increased effect22.
link







